A 67-year-old woman presented to her general practitioner with a swelling in her neck. It had been present for 4C5 years and had not changed in size during that time. She was completely asymptomatic and remained well.
On examination, there was a nodular goitre and no lymphadenopathy.
Investigations:
serum thyroid-stimulating hormone1.1 mU/L (0.4C5.0)
A subsequent ultrasound scan demonstrated seven nodules bilaterally (ranging in size from 5 mm to 15 mm), which had no suspicious features.
What is the most appropriate next step in management according to British Thyroid Association 2014 Guidelines for the Management of Thyroid Cancer?
- A . fine-needle aspiration of largest nodule
- B . levothyroxine 100 micrograms daily
- C . radioactive iodine
- D . reassure and discharge
- E . subtotal thyroidectomy
A 17-year-old boy with type 1 diabetes mellitus was admitted with diabetic ketoacidosis precipitated by a recent viral illness.
Investigations on admission:
random plasma glucose15.0 mmol/L
arterial blood gases, breathing air:
pH7.07 (7.35C7.45)
H+85 nmol/L (35C45)
Investigations after initial treatment with fluids, insulin and potassium 7 h after admission:
random plasma glucose4.0 mmol/L
serum bicarbonate10 mmol/L (20C28)
At this stage, he was being given infusions of insulin (1 U/h) and glucose 5% (100 mL/h).
What is the most appropriate next step in management?
- A . continue current regimen
- B . continue current regimen but encourage oral carbohydrate intake
- C . continue insulin infusion and change glucose to a higher concentration
- D . give intravenous sodium bicarbonate
- E . stop insulin infusion if glucose falls any further, then repeat plasma glucose in 15 min
A 17-year-old boy had panhypopituitarism, including diabetes insipidus, following treatment for a craniopharyngioma. He was taking appropriate replacement therapy. In the transition clinic, he was keen to continue growth hormone replacement therapy following a 12-month break after reaching final height.
Which is the most appropriate test to assess his growth hormone status?
- A . clonidine test
- B . growth hormone day profile
- C . insulin-like growth factor 1
- D . insulin-like growth factor-binding protein 3
- E . insulin tolerance test
A 26-year-old woman with previously well-controlled primary hypothyroidism had been an in patient for treatment of an eating disorder for the previous 6 weeks. She had a history of anaemia resulting from multiple vitamin deficiency and gastric erosions. She had been taking levothyroxine 125 micrograms daily for the previous 5 years; since admission her medication had also included ferrous sulfate, calcium and vitamin D, and sucralfate. Her daily medicines were taken under supervision at 09.00 h. Although she was eating better and had gained 4 kg in weight, she was now complaining of tiredness and feeling "worse than ever".
On examination, she was thin, slightly pale and had no palpable goitre. Recent blood tests had confirmed that her anaemia had resolved.
Investigations:
serum corrected calcium2.28 mmo/L (2.20-2.60)
serum thryoid-stimulating hormone12.0 mU/L (0.4-5.0)
serum free T48.0 pmol/L (10.0-22.0)
serum T30.90 nmol/L (1.07-3.18)
What is the most appropriate next step in management?
- A . add liothyronine 20 micrograms daily
- B . administer levothyroxine alone at bedtime
- C . increase levothyroxine to 175 micrograms daily
- D . no change in treatment
- E . stop treatment with calcium and vitamin D
A 58-year-old man presented with tiredness and breathlessness. He had been treated for type 2 diabetes mellitus and hypertension for the past 10 years. He was free of complications. His current medication included ramipril 10 mg daily, rosuvastatin 10 mg daily, metformin 500 mg three times daily, dapagliflozin 10 mg once daily and exenatide 10 micrograms twice daily.
On examination, his body mass index was 36 kg/m2 (18C25).
Investigations:
haemoglobin93 g/L (130C180)
MCV110 fL (80C96)
white cell count3.6 ? 109/L (4.0C11.0)
platelet count140 ? 109/L (150C400)
reticulocyte count0.5% (0.5C2.4)
serum ferritin250 µg/L (15C300)
serum vitamin B1240 ng/L (160C760)
serum folate3.0 µg/L (2.0C11.0)
Which medication is most likely to be contributing to his anaemia?
- A . dapagliflozin
- B . exenatide
- C . metformin
- D . ramipril
- E . rosuvastatin
A 49-year-old woman presented with a slowly enlarging lump in her neck.
On examination, there was a 3.5-cm firm nodule in the left lobe of the thyroid gland, with no associated lymphadenopathy.
Investigations:
serum thyroid-stimulating hormone<0.05 mU/L (0.4C5.0)
serum free T426.0 pmol/L (10.0C22.0)
serum free T38.6 pmol/L (3.0C7.0)
An ultrasound scan showed an enlarged thyroid gland, with small nodules throughout. There was a larger hypoechoic 3.3-cm nodule with increased intranodular vascularity in the lower pole of the left lobe, with no associated lymphadenopathy.
What is the most appropriate management?
- A . core biopsy of the thyroid nodule
- B . fine-needle aspiration of the nodule
- C . isotope uptake scan
- D . partial thyroidectomy
- E . radioactive iodine treatment
A 16-year-old girl presented with primary amenorrhoea. In early childhood she had undergone an inguinal herniorrhaphy. She had no other medical history of note. There was a family history of infertility affecting a maternal aunt.
On examination, she had adult breast development but no pubic or axillary hair.
Examination was otherwise normal.
What test is most likely to aid diagnosis?
- A . blood karyotype
- B . MR scan of pituitary and olfactory bulbs
- C . ovarian antibody titres
- D . plasma gonadotropins
- E . ultrasound scan of pelvis
A 17-year-old girl was referred to the outpatient clinic with irritability, weight loss and
difficulty sleeping. At the age of 4, she had presented with rapid growth, breast development and vaginal bleeding. The results of a gonadotropin-releasing hormone (GnRH) stimulation test performed at that time are given below.
serum oestradiolplasma FSHplasma LH
(200C400 pmol/L)(2.5C10.0 U/L)(2.5C10.0 U/L)
0 min365<0.7<0.5
30 minC<0.7<0.5
60 minC<0.7<0.5
She had been treated with GnRH analogue until the age of 11 and puberty had then progressed normally.
On examination, she was found to be tremulous, tachycardic and hyper-reflexic. Several large, irregular café-au-lait spots were found.
Investigations:
serum thyroid-stimulating hormone<0.05 mU/L (0.4C5.0)
serum free T436.0 pmol/L (10.0C22.0)
What is the most likely diagnosis?
- A . Carney’s complex
- B . Cowden’s syndrome
- C . McCuneCAlbright syndrome
- D . multiple endocrine neoplasia type 2
- E . neurofibromatosis type 1
A 44-year-old man was referred for investigation of cortisol excess. He had poorly controlled hypertension, and a long history of type 2 diabetes mellitus with retinopathy and peripheral neuropathy. His medication comprised aspirin, ramipril, atenolol,
carbamazepine, metformin and simvastatin.
Initial investigations:
serum cortisol (09.00 h)350 nmol/L (200C700)
serum cortisol (22.00 h)48 nmol/L (50C250)
overnight dexamethasone suppression test (after 1 mg dexamethasone):
serum cortisol93 nmol/L (<50)
24-h urinary free cortisol (day 1)225 nmol (55C250)
24-h urinary free cortisol (day 2)200 nmol (55C250)
24-h urinary free cortisol (day 3)185 nmol (55C250)
What is the most appropriate next step in management?
- A . CT scan of adrenal glands
- B . dexamethasone-suppressed corticotrophin-releasing hormone test
- C . high-dose 48-h dexamethasone suppression test
- D . MR scan of pituitary
- E . reassure and discharge
A 33-year-old woman was seen for diabetes review 2 months after her first pregnancy. Diabetes mellitus had been diagnosed at 18 weeks’ gestation. She had experienced no symptoms; routine urinalysis had shown glucose 4+, with no ketones, and her fasting blood glucose concentration was 6.2 mmol/L (3.0C6.0), rising to 13.5 mmol/L (<7.8) in a 75-g oral glucose tolerance test. She had been treated with insulin during the pregnancy, and stopped after delivery. Her mother and maternal aunt had been treated for type 2 diabetes mellitus, and a maternal uncle for type 1 diabetes. Her body mass index was 23.7 kg/m2 (18C25).
Without insulin she remained well, with no osmotic symptoms, no weight loss and no ketosis.
Investigations:
fasting plasma glucose8.4 mmol/L (3.0C6.0)
haemoglobin A1c68 mmol/mol (20C42)
oral glucose tolerance test (75 g):
fasting plasma glucose7.9 mmol/L (3.0C6.0)
2-h plasma glucose13.8 mmol/L (<7.8)
serum insulin72 pmol/L (<186)
serum C-peptide945 pmol/L (180C360)
A trial of therapy with gliclazide 40 mg once daily led to a significant improvement in her blood glucose.
What is the most likely cause of her diabetes?
- A . latent autoimmune diabetes in adulthood
- B . maturity-onset diabetes of the young caused by glucokinase mutation
- C . maturity-onset diabetes of the young caused by HNF-1? mutation
- D . type 1 diabetes mellitus
- E . type 2 diabetes mellitus
A 64-year-old man was referred to the foot clinic. He had tripped over his cat 1 week previously and had complained of an ache in his left foot since then. He had a 12-year history of type 2 diabetes mellitus and hypertension. He was taking metformin, gliclazide, pioglitazone, bendroflumethiazide, ramipril, simvastatin and aspirin.
On examination, his blood pressure was 154/88 mmHg. Foot examination showed absent vibration perception to his ankle. The dorsalis pedis and posterior tibial pulses were easily palpable on both feet.
Investigations:
serum urea12.6 mmol/L (2.5C7.0)
serum creatinine166 µmol/L (60C110)
haemoglobin A1c79 mmol/mol (20C42)
urinary albumin:creatinine ratio8.7 mg/mmol (<2.5)
X-ray of left footsee image


What is the most appropriate initial management for this deformity?
- A . bed rest
- B . custom-made hospital footwear
- C . full contact plaster cast
- D . referral for urgent surgery
- E . removable aircast boot
A 34-year-old woman presented with palpitations, heat intolerance and a slight tremor. She was 9 weeks into her first pregnancy. She had not had any morning sickness.
On examination, her pulse was 100 beats per minute. She had a small uniform goitre but no tremor and no eye signs.
Investigations:
serum thyroid-stimulating hormone<0.01 mU/L (0.4C5.0)
serum free T442.0 pmol/L (10.0C22.0)
serum free T315.0 pmol/L (3.0C7.0)
anti-thyroid-stimulating hormone receptor
antibodies14 U/L (<7)
The decision was taken to treat her Graves’ disease with propylthiouracil (PTU) rather than carbimazole.
What is the reason for this decision?
- A . concordance with PTU is greater
- B . PTU does not cross the placenta
- C . PTU is less associated with agranulocytosis
- D . PTU is less associated with aplasia cutis
- E . PTU is less associated with hepatitis
A 58-year-old man was referred to the endocrine clinic after a CT scan of abdomen had shown a 4.5-cm left adrenal mass, with a Hounsfield unit measurement of 11 (consistent with high lipid content). He had a 10-year history of type 2 diabetes mellitus and was taking metformin. He was also taking atenolol for hypertension.
On examination at the clinic, his blood pressure was 162/94 mmHg. He was centrally obese with a body mass index of 27 kg/m2 (18C25).
Investigations:
serum potassium3.9 mmol/L (3.5C4.9)
plasma renin activity (after 30 min upright)1.0 pmol/mL/h (3.0C4.3)
plasma aldosterone (after 4 h upright)680 pmol/L (330C830)
overnight dexamethasone suppression test (after 1 mg dexamethasone):
serum cortisol164 nmol/L (<50)
24-h urinary free cortisol132 nmol (55C250)
24-h urinary catecholamines
(adrenaline and noradrenaline)normal
As the lesion was >4 cm in diameter, laparoscopic adrenalectomy was recommended.
What is the most appropriate advice to give to the surgical team about perioperative management?
- A . give corticosteroid cover during and after surgery and reassess postoperatively
- B . give preoperative ?-adrenergic receptor blockade in case the lesion is an occult phaeochromocytoma
- C . measure cortisol and aldosterone 2 weeks postoperatively
- D . no special precautions are required
- E . short tetracosactide (Synacthen®) test 48 h postoperatively
A 16-year-old boy was referred with concern about delayed puberty. His stature had been short as a child. He reported an increase in height at the age of 13, and had begun to develop pubic hair at the age of 14. He reported no further growth or development in the past year. His father recalled going through puberty at the age of 13.
On examination, his height was 1.60 m (between 0.4th and 2nd centile), weight was 56.4 kg (between 9th and 25th centile), genital development was Tanner stage 2 and testicular volume was 8 mL bilaterally. Pubic hair was Tanner stage 2, with no evidence of androgenic axillary hair. Bone age at the left wrist was 13.5 years.
Investigations:
serum testosterone2.9 nmol/L (9.0C35.0)
Which feature in his clinical presentation most strongly suggests a diagnosis other than constitutional delay?
- A . 2.5-year delay in bone age
- B . absence of axillary hair in the presence of pubic hair
- C . being below the 2nd centile for height
- D . discordance between the height centile and the weight centile
- E . failure to progress through puberty
A pregnant 36-year-old woman presented to the diabetes outpatient clinic. She had type 2 diabetes mellitus treated with diet, lifestyle changes and metformin 500 mg twice daily.
On examination, her blood pressure was 128/84 mmHg.
Investigations:
haemoglobin A1c47 mmol/mol (20C42)
urinary albumin: creatinine ratio1.6 mg/mmol (<3.5)
Which is the best agent to reduce the risk of pre-eclampsia in this patient?
- A . aspirin
- B . folic acid
- C . insulin
- D . labetalol
- E . omega-3-marine triglycerides
A 77-year-old woman presented with acute severe pain in the mid-thoracic spine after lifting a heavy bag of shopping. She had reported losing 6 cm in height over the preceding 5 years.
On examination, she was of slight build and experienced difficulty rising from a chair. There was tenderness in the region of T9/10.
Investigations:
plain thoracic X-ray of spinewedge fracture of T10
DXA scanT score C2.7 at L1CL4 and C2.3 at
the left total hip
What is the best estimate for the proportion of vertebral fractures that present clinically with back pain, as seen in this patient?
- A . <1%
- B . 5%
- C . 25%
- D . 60%
- E . 90%
A 61-year-old woman was referred to the blood pressure clinic because of refractory hypertension. One year previously, her blood pressure, urea and electrolytes had been normal. Her current therapy included verapamil modified-release 240 mg daily and doxazosin 16 mg daily.
On examination, she was 1.63 m tall and weighed 90 kg with an elevated waist to hip ratio.
Her blood pressure was 182/94 mmHg supine.
Investigations:
serum sodium137 mmol/L (137C144)
serum potassium2.8 mmol/L (3.5C4.9)
serum creatinine79 µmol/L (60C110)
plasma renin activity (after 30 min supine)<1.1 pmol/mL/h (1.1C2.7)
plasma aldosterone (after 30 min supine)<135 pmol/L (135C400)
What is the most appropriate investigation?
- A . 24-h urinary electrolytes
- B . 24-h urine to assess free cortisol: cortisone ratio
- C . analysis of the SCNN1B and SCNN1G genes
- D . overnight dexamethasone suppression test
- E . repeat renin and aldosterone concentrations after stopping verapamil for 2 weeks
A 36-year-old man of South Asian origin presented acutely with a widespread pruritic rash involving the extensor surfaces of the limbs.
On examination, he was moderately obese with a body mass index of 33 kg/m2 (18C25), and the rash was erythematous, with multiple small papules with yellow centres.
Investigations:
fasting plasma glucose11.0 mmol/L (3.0C6.0)
haemoglobin A1c109 mmol/mol (20C42)
serum cholesterol8.0 mmol/L (<5.2)
serum HDL cholesterol0.80 mmol/L (>1.55)
fasting serum triglycerides31.00 mmol/L (0.45C1.69)
What is the most likely diagnosis?
- A . dermatitis herpetiformis
- B . eruptive xanthoma
- C . granuloma annulare
- D . nodular prurigo
- E . tinea cutis
A 37-year-old woman presented with a 2-year history of increasingly frequent flushing episodes. She described alternating loose bowel motions and constipation. She had also noted menstrual irregularity. She had no respiratory symptoms. She denied headache or chest pain, but complained of palpitations.
On examination, she appeared well. Her blood pressure was 128/82 mmHg.
Investigations:
serum thyroid-stimulating hormone0.8 mU/L (0.4C5.0)
What is the most appropriate next investigation?
- A . fasting plasma gut hormones
- B . plasma metanephrines
- C . serum gonadotrophins
- D . urinary 5-hydroxyindoleacetic acid
- E . urinary metanephrines
A 26-year-old woman presented with recurrent Graves’ disease. After discussing the treatment options, she chose radioiodine.
What dose of radioiodine is most appropriate in uncomplicated Graves’ disease?
- A . 100C200 MBq
- B . 400C600 MBq
- C . 700C900 MBq
- D . 1000C1200 MBq
- E . 1400C1600 MBq
A 29-year-old woman presented with primary infertility, having had unprotected sexual intercourse for 15 months. Menarche had occurred at the age of 13.5 years. Her menstrual cycle was irregular, occurring every 20C60 days. There was no history of galactorrhoea. She denied abnormal hair growth.
On examination, her body mass index was 28.9 kg/m2 (18C25) and she had normal secondary sexual characteristics. Her visual fields were full to confrontation.
Investigations:
serum androstenedione12.8 nmol/L (0.6C8.8)
serum oestradiol205 pmol/L (200C400)
serum testosterone2.4 nmol/L (0.5C3.0)
serum sex hormone binding globulin23 nmol/L (40C137)
serum follicle-stimulating hormone4.3 U/L (2.5C10.0)
serum luteinising hormone8.5 U/L (2.5C10.0)
serum prolactin420 mU/L (<360)
hysterosalpingogrampatent fallopian tubes
partner’s semen analysisnormal sperm count and motility
What is the most appropriate first-line intervention?
- A . cabergoline
- B . human chorionic gonadotropin
- C . human menopausal gonadotropins
- D . metformin
- E . orlistat
A 66-year-old woman was admitted with carpopedal spasm. During the previous week she had had 2 days of diarrhoea following treatment with ciprofloxacin for a urinary tract infection. She had long-standing rheumatoid arthritis treated with prednisolone 5 mg daily, and was also taking alendronic acid, omeprazole and furosemide.
Investigations:
serum creatinine115 ?mol/L (60C110)
serum corrected calcium1.79 mmol/L (2.20C2.60)
serum alkaline phosphatase124 U/L (45C105)
serum magnesium0.26 mmol/L (0.75C1.05)
plasma parathyroid hormone2.7 pmol/L (0.9C5.4)
Which medicine is most likely to be responsible for her metabolic derangement?
- A . alendronic acid
- B . ciprofloxacin
- C . furosemide
- D . omeprazole
- E . prednisolone
A 48-year-old man presented with gynaecomastia. His serum oestradiol was increased and
a CT scan of adrenal glands revealed a 13-cm tumour of the left adrenal gland. Further workup showed increased secretion of 17-hydroxyprogesterone, cortisol and androstenedione. A diagnosis of adrenocortical carcinoma was suspected.
Investigations:
staging CT scan of chest and abdomenno evidence of metastasis
What is the most appropriate next step in management?
- A . adrenal fine-needle biopsy
- B . iodocholesterol scan
- C . left adrenalectomy followed by adjuvant combination chemotherapy
- D . left adrenalectomy followed by adjuvant mitotane treatment
- E . MR scan of adrenal glands with chemical shift analysis
An 18-year-old man with cystic fibrosis was referred to clinic. Over recent months his lung function had deteriorated and he had lost weight. He was being treated for a chest infection at the time of the consultation.
Investigations:
oral glucose tolerance test (75 g):
fasting plasma glucose8.2 mmol/L (3.0C6.0)
2-h plasma glucose13.5 mmol/L (<7.8)
What is the most appropriate management?
- A . repeat oral glucose tolerance test after chest infection has resolved
- B . restrict refined carbohydrate intake
- C . start gliclazide
- D . start insulin
- E . start sitagliptin
A 55-year-old man presented with a 3-year history of increasing pain in the right hip. He had been otherwise well and was taking no medication. He was reluctant to consider any intravenous treatment as he had a phobia of needles.
Investigations:
X-ray of hipssclerotic bone in right pubis and ischium
suggestive of Paget’s disease
What is the most appropriate oral treatment?
- A . calcium and vitamin D
- B . ibandronate sodium
- C . risedronate sodium
- D . sodium clodronate
- E . strontium ranelate
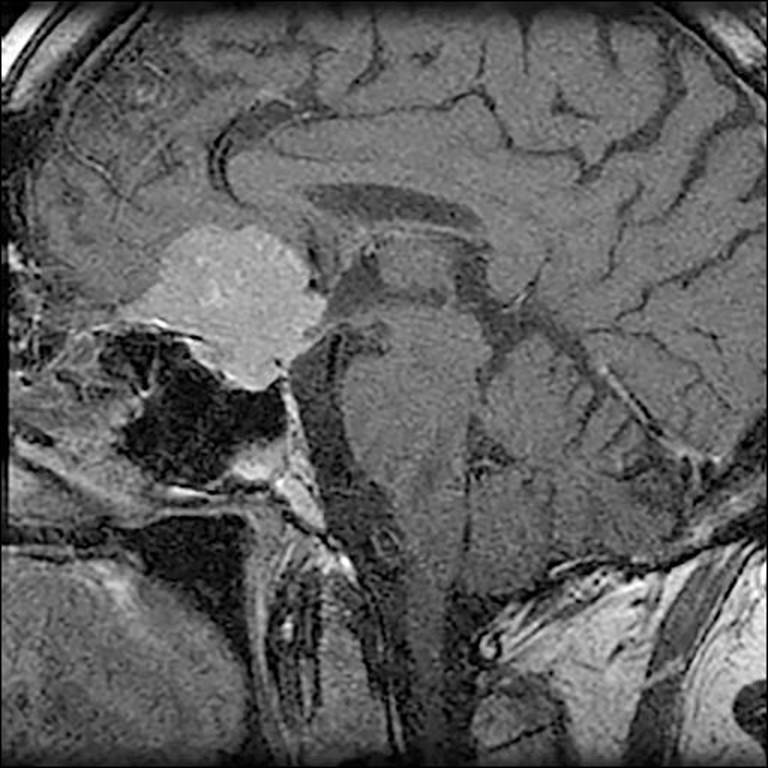
A 26-year-old woman was urgently referred to clinic with a 6-week history of retroorbital headaches and deteriorating vision. Her past medical history was unremarkable, although on questioning she admitted that she had recently found it increasingly difficult to cope with her busy job.
On examination, her pulse was 60 beats per minute and regular, and her blood pressure was 110/75 mmHg lying and 90/60 mmHg standing. She was pale and had dry skin. Visual acuities were reduced (6/12 right; 6/24 left), and she had a bitemporal inferior quadrantanopia.
Investigations:
serum sodium132 mmol/L (137C144)
serum potassium4.0 mmol/L (3.5C4.9)
short tetracosactide Synacthen® test (250 micrograms):
serum cortisol (30 min after tetracosactide)185 nmol/L (>550)
plasma follicle-stimulating hormone2.7 U/L
plasma luteinising hormone3.5 U/L
serum prolactin1050 mU/L (<360)
serum thyroid-stimulating hormone0.3 mU/L (0.4C5.0)
serum free T48.0 pmol/L (10.0C22.0)
serum insulin-like growth factor 14.7 nmol/L (7.5C37.3)
MR scan of brainsee image


What is the most likely diagnosis?
- A . autoimmune hypophysitis
- B . craniopharyngioma
- C . non-functioning pituitary adenoma
- D . prolactinoma
- E . Rathke’s cleft cyst
A 23-year-old woman was found to have type 1 diabetes mellitus following a short history of polyuria, polydipsia and unintentional weight loss. She started taking insulin aspart before meals and insulin detemir daily.
What is the most appropriate time from diagnosis to start screening for microalbuminuria?
- A . 1 year
- B . 2 years
- C . 5 years
- D . 10 years
- E . immediately
A 64-year-old man presented with palpitations, fatigue and malaise. Two months previously, he had sustained an acute myocardial infarction complicated by ventricular tachycardia and cardiac arrest, and had been discharged taking amiodarone 200 mg daily.
On examination, he appeared well, his pulse was 90 beats per minute and regular, and he had mild tremor of his hands but no other abnormal signs.
Investigations:
serum thyroid-stimulating hormone6.2 mU/L (0.4C5.0)
serum free T418.2 pmol/L (10.0C22.0)
serum free T34.8 pmol/L (3.0C7.0)
What is the most appropriate next step in management?
- A . discontinue amiodarone
- B . isotope scan of thyroid
- C . repeat thyroid function tests in 2 months
- D . repeat thyroid function tests in 12 months
- E . start levothyroxine
A 64-year-old woman presented with features of acromegaly. An MR scan showed a pituitary tumour with cavernous sinus extension. She underwent trans-sphenoidal surgery and histology of the pituitary tissue showed numerous cells immunostaining for growth hormone.
Investigations (6 months postoperatively):
MR scan of pituitaryenlarged sella, residual tumour in right cavernous sinus
serum growth hormone (day curve average)3.2 ?g/L (<2)
serum insulin-like growth factor 142.0 nmol/L (3.3C23.3)
What is the most appropriate next step in management?
- A . conventional external beam radiotherapy to pituitary region
- B . long-acting octreotide
- C . pegvisomant
- D . repeat trans-sphenoidal surgery
- E . watchful waiting
A 17-year-old Caucasian girl presented with primary amenorrhea.
On examination, her body mass index was 21 kg/m2 (18C25). Her body habitus was normal and she had appropriate breast development. There was no hirsutism or acne.
Investigations:
serum oestradiol<180 pmol/L (200C400)
serum testosterone31.7 nmol/L (0.5C3.0)
serum follicle-stimulating hormone4.0 U/L (2.5C10.0)
serum luteinising hormone6.0 U/L (2.5C10.0)
What is the most likely diagnosis?
- A . adrenocortical carcinoma
- B . androgen-secreting ovarian tumour
- C . complete androgen insensitivity syndrome
- D . ovarian hyperthecosis
- E . polycystic ovary syndrome
A 64-year-old man was reviewed in the diabetes clinic. He had a history of type 2 diabetes mellitus treated for 12 years. He had sustained a previous episode of acute kidney injury believed to be secondary to renal artery stenosis and exposure to an ACE inhibitor. He was being treated with metformin 500 mg three times daily and gliclazide 80 mg twice daily.
Investigations:
serum sodium143 mmol/L (137C144)
serum potassium4.4 mmol/L (3.5C4.9)
serum creatinine123 µmol/L (60C110)
estimated glomerular filtration rate (MDRD)51 mL/min/1.73 m2 (>60)
haemoglobin A1c75 mmol/mol (20C42)
He required a third drug that would not require dose adjustment if renal function were to decline in the future.
What additional medication is most appropriate?
- A . alogliptin
- B . linagliptin
- C . saxagliptin
- D . sitagliptin
- E . vildagliptin
An 18-year-old man presented to the thyroid clinic complaining of a lump in his neck that had been present for 9 weeks. It was not painful. At the age of 12, he had developed acute lymphoblastic leukaemia and had undergone a bone marrow transplant preceded by total body irradiation and cyclophosphamide.
On examination, he was euthyroid. There was a 1.5-cm firm mass on the left side of the neck, which moved when he swallowed.
Investigations:
serum thyroid-stimulating hormone1.9 mU/L (0.4C5.0)
serum free T416.8 pmol/L (10.0C22.0)
What is the most appropriate initial course of action?
- A . CT scan of neck and thorax
- B . FDG-PET-CT scan
- C . surgical referral for hemithyroidectomy
- D . technetium-99m scintigraphy scan of thyroid
- E . ultrasound-guided fine-needle aspiration of the nodule
A 16-year-old boy was referred to the diabetes clinic following the discovery of a random plasma glucose concentration of 18.0 mmol/L. His general practitioner had begun treatment with metformin. The patient had a body mass index of 35 kg/m2 (18C25). He had had problems throughout his childhood, and had been taken out of school and was educated at home by his mother. He was attending the ophthalmology clinic for visual problems.
On examination, he was obese. He had hearing aids in both ears and evidence of acanthosis nigricans. Neither parent had a history of diabetes mellitus.
What is the most likely diagnosis?
- A . Alström’s syndrome
- B . BardetCBiedl syndrome
- C . hepatocyte nuclear factor 1? mutation
- D . mitochondrial diabetes
- E . type 2 diabetes mellitus
A 26-year-old woman was recovering from diabetic ketoacidosis and had been switched to her usual basal bolus insulin regimen. Her capillary blood glucose measurements during the day were high but fasting plasma glucose was in the range 5.0C7.0 mmol/L (3.0C6.0). She was drinking and eating normally.
On examination, her pulse was 76 beats per minute and her blood pressure was 106/66 mmHg. Urinalysis showed ketones 1+.
Investigations:
serum sodium143 mmol/L (137C144)
serum potassium4.4 mmol/L (3.5C4.9)
serum bicarbonate22 mmol/L (20C28)
serum creatinine72 µmol/L (60C110)
plasma glucose 2 h after breakfast21 mmol/L
What is the most appropriate next step in management?
- A . change to twice daily pre-mixed insulin
- B . increase basal insulin at bed time
- C . increase bolus insulin with meal
- D . start glucose 5% with intravenous insulin
- E . start variable-rate intravenous insulin infusion
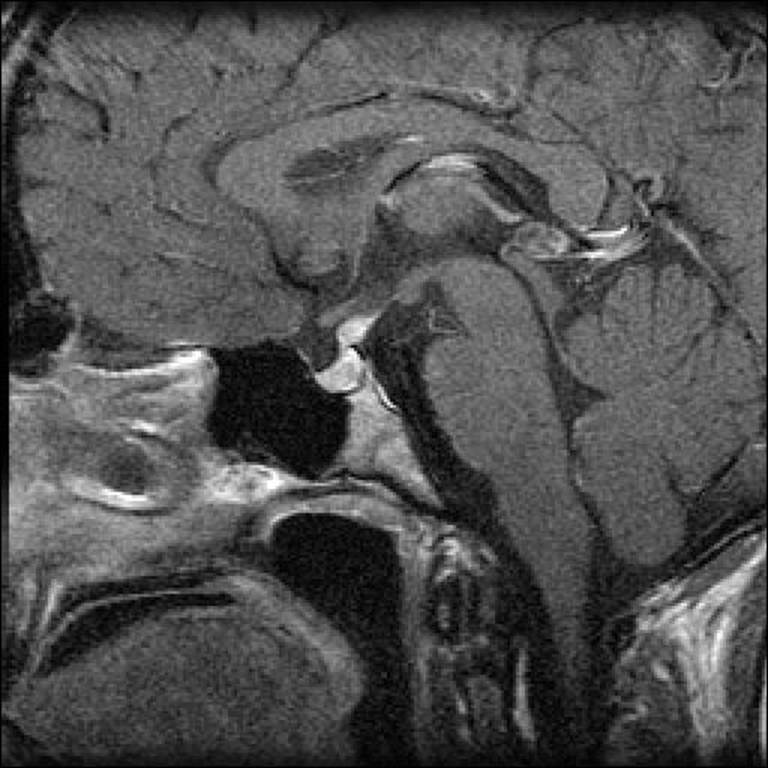
A 56-year-old man was referred urgently by an ophthalmologist after presenting with a 6-month history of deteriorating vision. The patient had a 40 pack-year smoking history. Before his vision problem, he had never visited his general practitioner.
Investigations:
serum cortisol (09.00 h)389 nmol/L (200C700)
serum testosterone8.6 nmol/L (9.0C35.0)
plasma follicle-stimulating hormone2.1 U/L (1.0C7.0)
plasma luteinising hormone2.4 U/L (1.0C10.0)
serum prolactin896 mU/L (<360)
serum thyroid-stimulating hormone1.4 mU/L (0.4C5.0)
MR scan of pituitarysee image

What is the most likely diagnosis?
- A . craniopharyngioma
- B . meningioma
- C . non-functioning adenoma
- D . prolactinoma
- E . Rathke’s cyst
A 32-year-old woman, with a 22-year history of type 1 diabetes mellitus, was seen in a pre-pregnancy diabetes clinic. She was a primigravida.
On examination, she had early background retinopathy, her blood pressure was 128/68
mmHg, and her body mass index was 29.7 kg/m2 (18C25).
Investigations:
haemoglobin A1c56 mmol/mol (20C42)
urinary albumin:creatinine ratio1.2 mg/mmol (<3.5)
Over the years her haemoglobin A1c concentration had varied between 58 and 69 mmol/mol. She had impaired awareness of hypoglycaemia and experienced approximately two severe hypoglycaemic events per year. She was worried about the risk of severe congenital malformations in her baby.
To what extent will the average risk of severe congenital malformation be increased in infants born to this mother with pregestational diabetes?
- A . two-fold
- B . four-fold
- C . six-fold
- D . eight-fold
- E . ten-fold
A 32-year-old woman with a recurrent history of Graves’ thyrotoxicosis was being considered for radioiodine treatment. However, she wanted to conceive again at some stage and asked how soon she could become pregnant.
After what minimum interval would it be safe for her to conceive again?
- A . 2 months
- B . 4 months
- C . 6 months
- D . 8 months
- E . 12 months
A 26-year-old man presented urgently, complaining of muscle pains. He had been found to have heterozygous familial hypercholesterolaemia 2 years previously owing to a mutation in the PCSK9 gene. He had a strong family history of premature vascular disease. He was taking atorvastatin 80 mg daily.
Investigations:
serum creatine kinase2782 U/L (24C195)
serum cholesterol5.7 mmol/L (<5.2)
After stopping atorvastatin, his serum creatine kinase fell to within the normal range.
What is the most appropriate next step in management?
- A . restart atorvastatin 10 mg
- B . restart atorvastatin 40 mg
- C . start ezetimibe 10 mg
- D . start fenofibrate 100 mg
- E . start fluvastatin 40 mg
A 26-year-old man with type 1 diabetes mellitus attended a carbohydrate-counting course to facilitate tighter glucose control. He estimated that his carbohydrate ratio was 1:10 and 1 unit correction dose reduced his glucose by 3.0 mmol/L.
He planned to eat a meal containing 50 g of carbohydrate. His pre-meal glucose was 16.0 mmol/L with a target blood glucose of 7.0 mmol/L.
What is the correct dose of bolus insulin (units) that he should administer?
- A . 2
- B . 4
- C . 6
- D . 8
- E . 10
A 47-year-old nuclear physics professor was referred for advice before taking up an overseas position, overseeing the dismantling of a reactor at the site of a recent nuclear accident. She stated that she would face a small risk of being exposed to significant radioactive contamination during her work and was concerned about her future risk of thyroid cancer.
What is the most appropriate advice?
- A . avoid consuming local milk and vegetables
- B . no precautions are necessary for people aged 40 years or over
- C . take potassium iodide tablets
- D . take selenium tablets
- E . wear lead neck shield while outdoors
A 36-year-old woman was referred to the endocrine clinic with abnormal thyroid function tests. She gave a 3-year history of increased sweating and anxiety following an assault and, initially, her symptoms had been attributed to post-traumatic stress disorder.
Investigations:
serum thyroid-stimulating hormone (TSH)3.1 mU/L (0.4C5.0)
serum free T429.8 pmol/L (10.0C22.0)
serum free T33.5 pmol/L (3.0C7.0)
What is the most likely interpretation of her thyroid function test results?
- A . assay interference
- B . factitious thyrotoxicosis
- C . resistance to thyroid hormone
- D . TSH-secreting pituitary adenoma
- E . use of combined oral contraceptive pill
A 72-year-old woman presented with a painless swelling in the front of the neck, which she had first noticed 2C3 months previously. She was otherwise well, with no symptoms of mass effect in her neck, and was not taking any medication.
On examination, her thyroid gland was moderately enlarged, and felt uniformly nodular. There was no associated lymphadenopathy. Her pulse was 78 beats per minute and regular, and there were no signs of thyrotoxicosis.
Investigations:
serum thyroid-stimulating hormone<0.01 mU/L (0.4C5.0)
serum free T424.8 pmol/L (10.0C22.0)
serum free T310.3 pmol/L (3.0C7.0)
technetium-99m scan of thyroid (20-min uptake)patchy uptake in both thyroid lobes
What is the most appropriate management?
- A . carbimazole plus levothyroxine
- B . partial thyroidectomy
- C . radioiodine
- D . repeat thyroid function tests after 6 months
- E . total thyroidectomy
A 41-year-old man presented to his general practitioner with symptoms of palpitations, sweating and anxiety. His blood pressure was 160/102 mmHg. He was advised to take propranolol 40 mg twice daily but was admitted to hospital later that week with an episode of pulmonary oedema.
On examination at the time of admission, he was noted to be pale and sweating and he had a blood pressure of 210/124 mmHg. A phaeochromocytoma was suspected.
What is the most likely cause of the cardiovascular deterioration following administration of propranolol?
- A . ?1-adrenoceptor blockade leading to acute left ventricular dysfunction
- B . inadequate ?-adrenoceptor blockade because of the short half-life of the drug
- C . inhibition of catechol-O-methyltransferase by propranolol leading to an increase in circulating noradrenaline
- D . loss of ?2-adrenoceptor-mediated vasodilatation
- E . propranolol acting as an agonist at ?1-adrenoceptors
A 55-year-old man with mild polyuria and tiredness was seen on a renal ward. He had had a living-related kidney transplant 6 months previously. He had good graft function while being treated with prednisolone 5 mg daily, mycophenolate mofetil 1 g twice daily and tacrolimus 3 mg twice daily. He was also taking atenolol 50 mg daily and simvastatin 40 mg daily.
Investigations:
haemoglobin A1c75 mmol/mol (20C42)
random plasma glucose18.0 mmol/L
Which drug is most likely to be responsible for his diabetes of new onset?
- A . atenolol
- B . mycophenolate mofetil
- C . prednisolone
- D . simvastatin
- E . tacrolimus
A 45-year-old woman was found to be hypertensive by her general practitioner. She was otherwise well and was not taking any medication. However, she regularly ate health food containing liquorice. There was no family history of significant illness.
On examination, her blood pressure was 170/110 mmHg.
Investigations:
serum sodium140 mmol/L (137C144)
serum potassium3.8 mmol/L (3.5C4.9)
serum creatinine70 µmol/L (60C110)
plasma renin activity (after 30 min supine)0.5 pmol/mL/h (1.1C2.7)
plasma aldosterone (after 30 min supine)450 pmol/L (135C400)
During the investigations, her blood pressure was controlled with doxazosin.
What is the most likely diagnosis?
- A . apparent mineralocorticoid excess
- B . Gitelman’s syndrome
- C . primary hyperaldosteronism
- D . pseudohyperaldosteronism
- E . renal artery stenosis
Carbimazole is routinely used in the management of thyroid disease.
What does carbimazole inhibit?
- A . deiodinase type 1
- B . presentation of thyroid antigens to autoreactive T cells
- C . sodium/iodide symporter
- D . thyroglobulin synthesis
- E . thyroid peroxidase
A 76-year-old woman with type 2 diabetes mellitus was reviewed. Treatment with thiazolidinedione was being considered, but she was worried about the effect this medication might have on the incidence of complications. She had known background retinopathy.
What complication is more likely to worsen in a patient taking a thiazolidinedione?
- A . cataract
- B . hard exudates
- C . macular oedema
- D . retinal haemorrhages
- E . retinal vein thrombosis
A 64-year-old man attended the diabetes clinic for annual review. He complained of very recent tingling in his feet. A monofilament was used to screen for the presence of chronic sensorimotor diabetic peripheral neuropathy.
What force should a monofilament deliver?
- A . 1 g
- B . 2 g
- C . 5 g
- D . 10 g
- E . 20 g
A 37-year-old man, who had previously undergone female-to-male gender reassignment surgery, attended the endocrine clinic for annual review. He had no complaints and was happy with the results of his treatment. His medication consisted of testosterone undecanoate 1 g intramuscularly every 3 months.
What variable is it most important to monitor?
- A . fasting plasma glucose
- B . haematocrit
- C . serum luteinising hormone
- D . serum prostate-specific antigen
- E . serum testosterone
A 19-year-old man presented with late development of his pubic and axillary hair. He was otherwise well and was not taking any medication. His serum testosterone concentration had been normal on two previous occasions.
On examination, he now had post-pubertal secondary sexual characteristics. He had 15C20 mL testes.
Investigations:
serum testosterone27.0 nmol/L (9.0C35.0)
serum sex hormone binding globulin28 nmol/L (10C62)
serum follicle-stimulating hormone2.0 U/L (1.0C7.0)
serum luteinising hormone2.9 U/L (1.0C10.0)
What is the chief product of the Sertoli cell?
- A . anti-Müllerian hormone
- B . kisspeptin
- C . oestrogen
- D . serum sex hormone binding globulin
- E . testosterone
A 72-year-old man with a dense residual hemiparesis and unsafe swallow was fed via a percutaneous gastrostomy for 20 hours each day. He had type 2 diabetes mellitus that had been well controlled with metformin.
His glucose levels were uncontrolled on metformin powder at maximum dose.
According to the Joint British Diabetes Societies Guidelines (2012), what is the most appropriate next hypoglycaemic agent?
- A . exenatide
- B . gliclazide
- C . insulin detemir
- D . insulin glargine
- E . premixed (30/70) human insulin
A 23-year-old barmaid presented with headache, sweating and collapse. She had a past medical history of tension headache and unexplained abdominal pain. Her regular medication included amitriptyline 25 mg at night and paracetamol 1 g as required. She was a smoker and regularly drank alcohol.
On examination, her pulse was 120 beats per minute and her blood pressure was 210/128 mmHg.
Investigations:
24-h urinary metanephrine5.4 µmol (<2)
24-h urinary normetanephrine15.2 µmol (<3)
What substance is most likely to cause assay interference in the measurement of urinary metanephrines?
- A . alcohol
- B . amitriptyline
- C . caffeine
- D . nicotine
- E . paracetamol
A 16-year-old Caucasian girl presented with a 4-year history of facial hair growth, acne and secondary amenorrhoea.
On examination, her body mass index was 20 kg/m2 (18C25). Her gums and palmar creases were pigmented. Facial hair was evident on her upper lip and chin, and terminal hair was evident on her chest and abdomen. Her FerrimanCGallwey score was 25. She had acne affecting her face and back.
Investigations:
serum dehydroepiandrosterone sulphate15 µmol/L (3C12)
serum androstenedione12.2 nmol/L (0.6C8.8)
serum 17-hydroxyprogesterone120 nmol/L (1C10)
serum testosterone6.0 nmol/L (0.5C3.0)
serum sex hormone binding globulin18 nmol/L (40C137)
What treatment is likely to be of most benefit?
- A . cyproterone acetate
- B . fludrocortisone
- C . flutamide
- D . hydrocortisone
- E . metformin
A 26-year-old physiologist was seen in the diabetes outpatient clinic. She had type 1 diabetes mellitus of 9 months’ duration, treated with subcutaneous insulin.
She asked what symptoms of hypoglycaemia she might experience.
In what order are responses to hypoglycaemia most likely to occur as blood glucose falls?
- A . autonomic, counter-regulatory hormones, neuroglycopenia
- B . autonomic, neuroglycopenia, counter-regulatory hormones
- C . counter-regulatory hormones, autonomic, neuroglycopenia
- D . counter-regulatory hormones, neuroglycopenia, autonomic
- E . neuroglycopenia, autonomic, counter-regulatory hormones
A 56-year-old man attended routine follow-up for treatment of hypogonadism of late onset. His only medication was testosterone undecanoate (1 g intramuscular injection, every 12 weeks). He had started this treatment 12 months previously and last received the injection 1 week before review.
Digital rectal examination was normal.
Investigations (baseline):
haemoglobin145 g/L (130C180)
haematocrit0.46 (0.40C0.52)
serum prostate-specific antigen0.6 µg/L (<4)
Investigations (12 months after treatment):
haemoglobin153 g/L (130C180)
haematocrit0.51 (0.40C0.52)
serum prostate-specific antigen5.1 µg/L (<4)
What is the most appropriate next step in management?
- A . check serum testosterone
- B . decrease testosterone injection frequency to 14 weeks
- C . reassure and repeat blood tests in 12 months
- D . refer for urological assessment
- E . stop testosterone therapy
An 18-year-old woman was referred by her general practitioner for further investigation of “funny turns” during which she developed palpitations, sweating, tremor, hunger, anxiety and paraesthesiae; all of these symptoms were relieved immediately by a sugary drink.
She was otherwise well and was not taking any regular medication. There was a family history of type 1 diabetes mellitus. A spontaneous hypoglycaemic episode had not been captured and she was admitted to the diabetes/endocrine ward for a 72-hour fast. Her renal function was normal.
After a 12-hour fast she experienced her typical symptoms. Urinalysis showed no urinary ketones.
Investigations after 12-h fast:
fasting plasma glucose 2.0 mmol/L (3.0C6.0)
plasma insulin56 pmol/L (<21 after hypoglycaemia)
serum C-peptide514 pmol/L (180C360)
What is the most appropriate next step in management?
- A . coeliac axis angiography
- B . MR scan of abdomen and pelvis to localise a mesenchymal tumour producing insulin-like growth factor 2
- C . MR scan of pancreas to localise an insulinoma
- D . obtain a careful history looking for access to exogenous insulin
- E . request a urinary sulphonylurea screen on sample obtained during the fast
A 32-year-old man presented with medullary thyroid cancer, treated by total thyroidectomy. He had a past history of primary hyperparathyroidism, treated by selective parathyroidectomy. Postoperatively, plasma calcitonin was undetectable and serum calcium was in the normal range.
Investigations:
RET genotypeheterozygote codon 634 C>T mutation
What is the most appropriate approach to annual screening for phaeochromocytoma?
- A . biochemical screening
- B . CT scan of adrenal glands
- C . MIBG scanning
- D . MR scan of adrenal glands
- E . octreotide scanning
A 54-year-old woman was referred for assessment of low bone mineral density. Three months previously, after complaining of bloating and flatulence, she had been found to have coeliac disease and had been started on a gluten-free diet. She had no history of fracture and had not lost height. There was no family history of osteoporosis. Her only medication was omeprazole.
Investigations:
serum corrected calcium2.42 mmol/L (2.20C2.60)
serum alkaline phosphatase122 U/L (45C105)
plasma parathyroid hormone7.9 pmol/L (0.9C5.4)
DXA scansee image
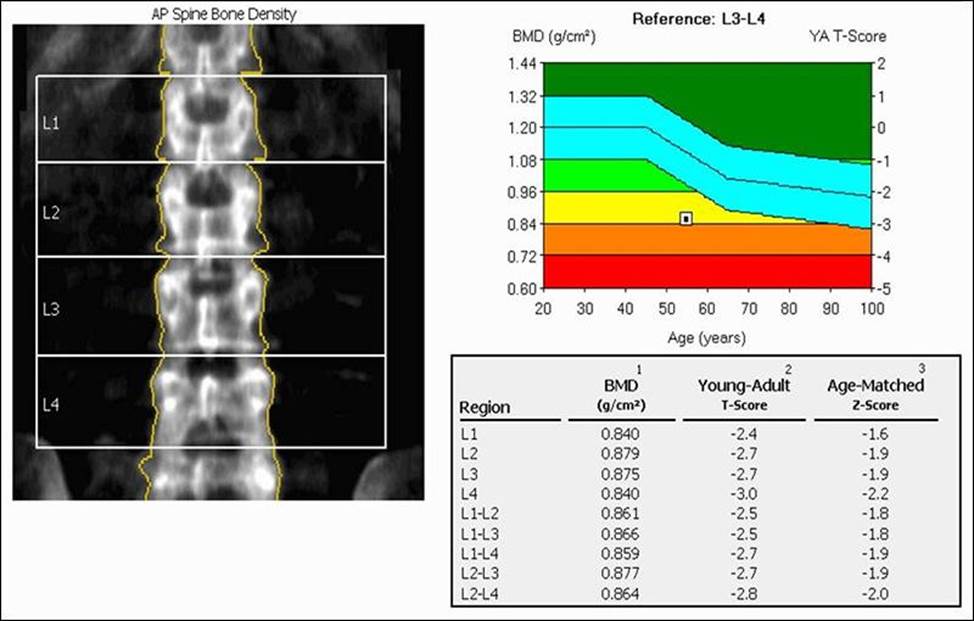

What is the most appropriate treatment?
- A . alendronic acid alone
- B . alendronic acid, and calcium and vitamin D
- C . calcium and vitamin D
- D . calcium and vitamin D, and intravenous zoledronic acid
- E . strontium ranelate
A 34-year-old woman with Addison’s disease reported four adrenal crises over the preceding 6 months, requiring hospital admission and intravenous administration of hydrocortisone. At outpatient follow-up, she was taking hydrocortisone 15 mg in the morning and 10 mg at midday, and fludrocortisone 50 micrograms daily.
What is the most important next step in management to prevent further crises?
- A . change to sustained-release hydrocortisone
- B . increase dosage of hydrocortisone
- C . measure plasma adrenocorticotropic hormone
- D . measure plasma renin
- E . measure post-dose 09.00 h cortisol
A 55-year-old dental nurse was referred for bone densitometry after sustaining a non-displaced fracture of the femur after falling down a step. She had experienced no other fractures. Her only medical problem was long-standing anaemia of unknown cause. The only family history was of persistent dental abscesses affecting her father. She had three children who were well. She was taking no medication.
Examination was normal.
Investigations:
haemoglobin102 g/L (115C165)
MCV85 fL (80C96)
white cell count6.0 ? 109/L (4.0C11.0)
platelet count245 ? 109/L (150C400)
erythrocyte sedimentation rate25 mm/1st h (<30)
serum creatinine85 µmol/L (60C110)
serum corrected calcium2.40 mmol/L (2.20C2.60)
serum alkaline phosphatase56 U/L (45C105)
DXA scan spine (L2CL4)T score +5.8
DXA scan total hipT score +5.4
What is the most likely diagnosis?
- A . fluorosis
- B . high bone mass phenotype
- C . myelodysplasia
- D . osteopetrosis
- E . Paget’s disease
A 46-year-old man of European descent was reviewed in the diabetes clinic. He had type 2 diabetes mellitus, which had been diagnosed 6 months previously. He had been symptom free and was a non-smoker but had a family history of cardiovascular disease. He exercised regularly and had managed to lose 8 kg.
On examination, his blood pressure was 148/76 mmHg, his weight was 76 kg and his body mass index was 24 kg/m2 (18C25).
Investigations:
urinary albumin:creatinine ratio0.6 mg/mmol (<2.5)
serum cholesterol5.6 mmol/L (<5.2)
serum HDL cholesterol0.90 mmol/L (>1.55)
fasting serum triglycerides2.20 mmol/L (0.45C1.69)
According to NICE guidelines (CG181, July 2014), what is the most appropriate management of his lipid profile?
- A . assess cardiovascular risk using UKPDS risk engine
- B . observe and repeat lipid profile in a few months
- C . start a fibrate
- D . start a statin
- E . start nicotinic acid
A 55-year-old woman presented with a 3-week history of nausea and vomiting. Her only medical complaints were frequent dyspepsia, for which she was taking indigestion tablets, and asthma for which she was taking a salbutamol inhaler as required.
On examination, there was no evidence of lymphadenopathy, her chest was clear on auscultation and abdominal examination was normal.
Investigations (before and after taking omeprazole for 3 weeks):
beforeafternormal
erythrocyte sedimentation rate (mm/1st h)44<30
serum creatinine (µmol/L)17011060C110
serum corrected calcium (mmol/L)2.852.402.20C2.60
serum phosphate (mmol/L)1.90.8C1.4
serum angiotensin-converting enzyme (U/L)8525C82
plasma parathyroid hormone (pmol/L)0.44.40.9C5.4
What is the most likely cause of the hypercalcaemia?
- A . milkCalkali syndrome
- B . multiple myeloma
- C . parathyroid hormone-related peptide-secreting malignancy
- D . primary hyperparathyroidism
- E . sarcoidosis
A 20-year-old man presented with a 6-month history of lethargy and weakness. His brother had been found to have adrenal failure at the age of 18. He had two sisters who were well and there was no other family history of endocrine autoimmune disease.
On examination, his blood pressure was 100/60 mmHg.
Investigations:
serum sodium136 mmol/L (137C144)
serum potassium4.8 mmol/L (3.5C4.9)
short tetracosactide (Synacthen®) test (250 micrograms):
baseline serum cortisol100 nmol/L
serum cortisol (30 min after tetracosactide)250 nmol/L (>550)
anti-adrenal antibodiesnegative
What is the most important diagnosis to consider?
- A . adrenoleucodystrophy
- B . autoimmune hypoadrenalism
- C . familial glucocorticoid resistance
- D . isolated adrenocorticotropic hormone deficiency
- E . tuberculosis
A 20-year-old man presented with a 6-month history of lethargy and weakness. His brother had been found to have adrenal failure at the age of 18. He had two sisters who were well and there was no other family history of endocrine autoimmune disease.
On examination, his blood pressure was 100/60 mmHg.
Investigations:
serum sodium136 mmol/L (137C144)
serum potassium4.8 mmol/L (3.5C4.9)
short tetracosactide (Synacthen®) test (250 micrograms):
baseline serum cortisol100 nmol/L
serum cortisol (30 min after tetracosactide)250 nmol/L (>550)
anti-adrenal antibodiesnegative
What is the most important diagnosis to consider?
- A . adrenoleucodystrophy
- B . autoimmune hypoadrenalism
- C . familial glucocorticoid resistance
- D . isolated adrenocorticotropic hormone deficiency
- E . tuberculosis
A 20-year-old man presented with a 6-month history of lethargy and weakness. His brother had been found to have adrenal failure at the age of 18. He had two sisters who were well and there was no other family history of endocrine autoimmune disease.
On examination, his blood pressure was 100/60 mmHg.
Investigations:
serum sodium136 mmol/L (137C144)
serum potassium4.8 mmol/L (3.5C4.9)
short tetracosactide (Synacthen®) test (250 micrograms):
baseline serum cortisol100 nmol/L
serum cortisol (30 min after tetracosactide)250 nmol/L (>550)
anti-adrenal antibodiesnegative
What is the most important diagnosis to consider?
- A . adrenoleucodystrophy
- B . autoimmune hypoadrenalism
- C . familial glucocorticoid resistance
- D . isolated adrenocorticotropic hormone deficiency
- E . tuberculosis
A 20-year-old man presented with a 6-month history of lethargy and weakness. His brother had been found to have adrenal failure at the age of 18. He had two sisters who were well and there was no other family history of endocrine autoimmune disease.
On examination, his blood pressure was 100/60 mmHg.
Investigations:
serum sodium136 mmol/L (137C144)
serum potassium4.8 mmol/L (3.5C4.9)
short tetracosactide (Synacthen®) test (250 micrograms):
baseline serum cortisol100 nmol/L
serum cortisol (30 min after tetracosactide)250 nmol/L (>550)
anti-adrenal antibodiesnegative
What is the most important diagnosis to consider?
- A . adrenoleucodystrophy
- B . autoimmune hypoadrenalism
- C . familial glucocorticoid resistance
- D . isolated adrenocorticotropic hormone deficiency
- E . tuberculosis
A 20-year-old man presented with a 6-month history of lethargy and weakness. His brother had been found to have adrenal failure at the age of 18. He had two sisters who were well and there was no other family history of endocrine autoimmune disease.
On examination, his blood pressure was 100/60 mmHg.
Investigations:
serum sodium136 mmol/L (137C144)
serum potassium4.8 mmol/L (3.5C4.9)
short tetracosactide (Synacthen®) test (250 micrograms):
baseline serum cortisol100 nmol/L
serum cortisol (30 min after tetracosactide)250 nmol/L (>550)
anti-adrenal antibodiesnegative
What is the most important diagnosis to consider?
- A . adrenoleucodystrophy
- B . autoimmune hypoadrenalism
- C . familial glucocorticoid resistance
- D . isolated adrenocorticotropic hormone deficiency
- E . tuberculosis
A 20-year-old man presented with a 6-month history of lethargy and weakness. His brother had been found to have adrenal failure at the age of 18. He had two sisters who were well and there was no other family history of endocrine autoimmune disease.
On examination, his blood pressure was 100/60 mmHg.
Investigations:
serum sodium136 mmol/L (137C144)
serum potassium4.8 mmol/L (3.5C4.9)
short tetracosactide (Synacthen®) test (250 micrograms):
baseline serum cortisol100 nmol/L
serum cortisol (30 min after tetracosactide)250 nmol/L (>550)
anti-adrenal antibodiesnegative
What is the most important diagnosis to consider?
- A . adrenoleucodystrophy
- B . autoimmune hypoadrenalism
- C . familial glucocorticoid resistance
- D . isolated adrenocorticotropic hormone deficiency
- E . tuberculosis
A 20-year-old man presented with a 6-month history of lethargy and weakness. His brother had been found to have adrenal failure at the age of 18. He had two sisters who were well and there was no other family history of endocrine autoimmune disease.
On examination, his blood pressure was 100/60 mmHg.
Investigations:
serum sodium136 mmol/L (137C144)
serum potassium4.8 mmol/L (3.5C4.9)
short tetracosactide (Synacthen®) test (250 micrograms):
baseline serum cortisol100 nmol/L
serum cortisol (30 min after tetracosactide)250 nmol/L (>550)
anti-adrenal antibodiesnegative
What is the most important diagnosis to consider?
- A . adrenoleucodystrophy
- B . autoimmune hypoadrenalism
- C . familial glucocorticoid resistance
- D . isolated adrenocorticotropic hormone deficiency
- E . tuberculosis
A 20-year-old man presented with a 6-month history of lethargy and weakness. His brother had been found to have adrenal failure at the age of 18. He had two sisters who were well and there was no other family history of endocrine autoimmune disease.
On examination, his blood pressure was 100/60 mmHg.
Investigations:
serum sodium136 mmol/L (137C144)
serum potassium4.8 mmol/L (3.5C4.9)
short tetracosactide (Synacthen®) test (250 micrograms):
baseline serum cortisol100 nmol/L
serum cortisol (30 min after tetracosactide)250 nmol/L (>550)
anti-adrenal antibodiesnegative
What is the most important diagnosis to consider?
- A . adrenoleucodystrophy
- B . autoimmune hypoadrenalism
- C . familial glucocorticoid resistance
- D . isolated adrenocorticotropic hormone deficiency
- E . tuberculosis
30-532
Results from an MR scan of pituitary are shown (see image).
What is the most likely diagnosis?
- A . autoimmune (lymphocytic) hypophysitis
- B . craniopharyngioma
- C . non-functioning pituitary adenoma
- D . psychogenic polydipsia
- E . Rathke’s cleft cyst
A 52-year-old man had been found to have type 1 diabetes mellitus at the age of 25. He had developed retinopathy at the age of 31 and a painless foot ulcer at the age of 40. His renal function had subsequently deteriorated.
On examination, urinalysis showed protein 1+, glucose 2+.
What is the most likely diagnosis?
- A . focal segmental glomerulosclerosis
- B . membranoproliferative glomerulonephritis
- C . minimal change glomerulonephritis
- D . nodular glomerulosclerosis
- E . tubulointerstitial nephritis
A 19-year-old man was seen in the diabetes clinic. He had lost 2 kg in weight since the diagnosis of diabetes mellitus 18 months previously. At presentation, his body mass index was 33 kg/m2 (18C25), his random plasma glucose was 18.0 mmol/L and his haemoglobin A1c was 56 mmol/mol (20C42). He was taking gliclazide, and metformin had been added later. His father and grandfather had developed diabetes mellitus during their twenties.
Investigations:
haemoglobin A1c56 mmol/mol (20C42)
serum C-peptide301 pmol/L (180C360)
anti-glutamic acid decarboxylase (GAD)
antibodiesnegative
What is the most likely diagnosis?
- A . chronic pancreatitis
- B . latent-onset diabetes of autoimmunity
- C . maturity-onset diabetes of the young
- D . type 1 diabetes mellitus
- E . type 2 diabetes mellitus
A 46-year-old South Asian man presented with a 2-month history of dry mouth and polyuria. He had hypertension treated with bendroflumethiazide. There was no family history of diabetes mellitus, but his father had died suddenly during lower limb angioplasty at the age of 51.
On examination, the patient’s pulse was 76 beats per minute and regular, and his blood pressure was 164/86 mmHg. The rest of the physical examination was normal. Urinalysis was normal.
Investigations:
serum sodium143 mmol/L (137C144)
serum potassium3.0 mmol/L (3.5C4.9)
serum creatinine123 µmol/L (60C110)
fasting plasma glucose6.9 mmol/L (3.0C6.0)
What is the most appropriate next step in management?
- A . change bendroflumethiazide to ramipril
- B . haemoglobin A1c measurement
- C . oral glucose tolerance test
- D . repeat fasting plasma glucose
- E . start oral hypoglycaemic treatment
A 35-year-old woman was referred with a left lower thyroid lesion. She was asymptomatic.
Examination confirmed the presence of a 2 ? 3-cm, firm, mobile, non-tender mass.
Investigations:
ultrasound-guided fine-needle aspiration biopsyThy 5
How is Thy 5 defined?
- A . abnormal, diagnostic of malignancy
- B . abnormal, suspicious (but not diagnostic of) malignancy
- C . follicular lesions
- D . non-diagnostic or inadequate
- E . non-neoplastic (consistent with nodular goitre or thyroiditis)
A 55-year-old woman presented complaining of difficulty losing weight.
On examination, her blood pressure was 170/105 mmHg and urinalysis showed protein 1+.
An ultrasound scan of abdomen revealed a 4.5-cm solid lesion in the right adrenal gland.
She was treated with ramipril and further endocrine evaluation was performed.
Investigations:
serum potassium3.6 mmol/L (3.5C4.9)
serum creatinine135 µmol/L (60C110)
plasma renin activity:
(after 30 min supine)3.9 pmol/mL/h (1.1C2.7)
(after 30 min upright)6.8 pmol/mL/h (3.0C4.3)
plasma aldosterone:
(after 30 min supine)150 pmol/L (135C400)
(after 4 h upright)350 pmol/L (330C830)
serum cortisol (09.00 h)650 nmol/L (200C700)
serum cortisol (22.00 h)225 nmol/L (50C250)
24-h urinary free cortisol230 nmol (55C250)
24-h urinary dopamine3200 nmol (<3100)
24-h urinary adrenaline120 nmol (<144)
24-h urinary noradrenaline450 nmol (<570)
What is the most appropriate initial management of the adrenal lesion?
- A . ?-adrenoceptor blockade
- B . angiotensin-2 receptor blockade
- C . medical observation with annual ultrasonography
- D . mineralocorticoid receptor blockade
- E . surgical excision
A 26-year-old woman was referred by her general practitioner for the management of subfertility. Her menarche had occurred at the age of 14 and she had experienced oligomenorrhoea since the age of 16. She also complained of gradually worsening hirsutism since puberty.
Clinical examination showed central obesity, a body mass index of 32 kg/m2 (18C25) and a blood pressure of 140/90 mmHg.
The following results were obtained within 1 week of her last menstrual period.
Investigations:
overnight dexamethasone suppression test (after 1 mg dexamethasone):
serum cortisol30 nmol/L (<50)
serum dehydroepiandrosterone sulphate12 µmol/L (3C12)
serum androstenedione10.0 nmol/L (0.6C8.8)
serum 17-hydroxyprogesterone38 nmol/L (1C10)
serum oestradiol200 pmol/L (200C400)
serum testosterone3.5 nmol/L (0.5C3.0)
serum sex hormone binding globulin30 nmol/L (40C137)
plasma follicle-stimulating hormone4.0 U/L (2.5C10.0)
plasma luteinising hormone6.0 U/L (2.5C10.0)
What is the most likely diagnosis?
- A . adrenal androgen-secreting tumour
- B . Cushing’s syndrome
- C . late-onset congenital adrenal hyperplasia
- D . ovarian androgen-secreting tumour
- E . polycystic ovary syndrome
A 16-year-old boy was referred to the endocrine clinic with symptoms of delayed puberty.
On examination, he had a reduced sense of smell, small-sized testes and underdeveloped secondary sexual characteristics.
Investigations:
serum testosterone3.5 nmol/L (9.0C35.0)
serum follicle-stimulating hormone1.0 U/L (1.0C7.0)
serum luteinising hormone1.5 U/L (1.0C10.0)
serum prolactin220 mU/L (<360)
MR scan of brainnormal
He asked about his future fertility.
What will be the most useful agent for him to achieve fertility?
- A . bromocriptine
- B . clomifene
- C . gonadotropin-releasing hormones
- D . octreotide
- E . testosterone
A 32-year-old man presented to the emergency department after becoming acutely unwell.
He had a 5-year history of type 1 diabetes mellitus and no other significant medical history.
On examination, he was apyrexial, his pulse was 120 beats per minute, his blood pressure was 96/58 mmHg and his respiratory rate was 32 breaths per minute.
Investigations:
random plasma glucose14.2 mmol/L
arterial blood gases, breathing 60% oxygen:
PO28.9 kPa (11.3C12.6)
PCO22.6 kPa (4.7C6.0)
pH7.10 (7.35C7.45)
H+79 nmol/L (35C45)
bicarbonate6.1 mmol/L (21C29)
base excessC18 mmol/L (±2)
What diagnosis is most likely to account for these results?
- A . acute asthma
- B . acute myocardial infarction
- C . diabetic ketoacidosis
- D . diabetic ketoacidosis and pulmonary embolism
- E . salicylate poisoning
An 80-year-old man was referred because of weight gain and low mood but said he was otherwise well. He had a complex cardiac history including a ventricular fibrillation arrest and a permanent pacemaker, but he had been very well for the past 3 years. He was taking amiodarone 100 mg daily, lisinopril 40 mg daily and furosemide 80 mg daily.
On examination, he had a pacemaker in situ and his pulse was 84 beats per minute and regular. He had a 2/6 mid-systolic murmur in the aortic area with no radiation, mild ankle oedema, and scanty basal crackles bilaterally on auscultation of his chest.
Investigations (before attending clinic):
serum thyroid-stimulating hormone19.0 mU/L (0.4C5.0)
serum free T411.0 pmol/L (10.0C22.0)
anti-thyroid peroxidase antibodies300 IU/mL (<50)
What is the most appropriate next step in management?
- A . review with repeat thyroid tests in 3 months
- B . start levothyroxine 25 micrograms daily
- C . start levothyroxine 100 micrograms daily
- D . start liothyronine sodium 10 micrograms twice daily
- E . stop amiodarone
A 17-year-old boy with a 10-year history of type 1 diabetes mellitus was admitted with
diabetic ketoacidosis after a night of binge drinking.
He was treated appropriately with a fixed-rate intravenous insulin infusion and intravenous sodium chloride 0.9%.
Twenty-four hours after admission, he was eating and drinking normally. He was taking his usual doses of subcutaneous insulin and his urinary ketones were undetectable.
Investigations (6 hours previously):
venous blood gases, breathing air:
PO25.6 kPa
PCO23.8 kPa
pH7.29
bicarbonate16 mmol/L
base excessC1 mmol/L
lactate1.1 mmol/L
What is the likely most cause of these results?
- A . alcohol toxicity
- B . concurrent aspirin ingestion
- C . continued ketonaemia
- D . hyperchloraemia
- E . hyporeninaemic hypoaldosteronism
A 46-year-old Afro-Caribbean man with sarcoidosis was found to have hypercalcaemia and was treated with prednisolone 20 mg/day. Within 3 weeks his serum calcium had fallen to within the reference range.
How do glucocorticoids reduce serum calcium in sarcoidosis?
- A . direct calcium shift into cells
- B . increase intravascular fluid volume
- C . promote urinary calcium excretion
- D . reduces extrarenal 1-?-hydroxylase activity
- E . suppress parathyroid hormone secretion
A 24-year-old man was referred for investigation of infertility. He had been having unprotected intercourse with his partner for 18 months, but the couple had failed to conceive. He had been treated for Hodgkin’s lymphoma at the age of 17.
What is the most appropriate investigation?
- A . semen analysis
- B . serum follicle-stimulating hormone
- C . serum inhibin
- D . serum testosterone
- E . testicular biopsy
A 55-year-old male-to-female transsexual was reviewed in clinic. She lived as a woman but had not undergone gender reassignment surgery. She was treated with cyproterone acetate 50 mg twice daily and estradiol 2 mg twice daily.
What are the most important tests for monitoring safe replacement?
- A . lipid profile and liver function tests
- B . lipid profile and serum prostate-specific antigen
- C . liver function tests and full blood count
- D . liver function tests and serum prostate-specific antigen
- E . serum prostate-specific antigen and full blood count
A 17-year-old girl presented with primary amenorrhoea. She had grown and developed normally. There was no history of galactorrhoea or hirsutism.
On examination, her height was 1.69 m, her weight was 68.3 kg, and her body mass index was 23.9 kg/m2 (18C25). She had stage 5 breast development and stage 5 pubic hair. Her visual fields were full to confrontation.
Investigations:
serum cortisol (09.00 h)416 nmol/L (200C700)
serum oestradiol51 pmol/L (200C400)
serum follicle-stimulating hormone0.8 U/L (2.5C10.0)
serum luteinising hormone1.2 U/L (2.5C10.0)
serum thyroid-stimulating hormone1.2 mU/L (0.4C5.0)
serum free T415.6 pmol/L (10.0C22.0)
What is the most appropriate next investigation?
- A . karyotyping
- B . luteinising hormone-releasing hormone test
- C . serum insulin-like growth factor 1
- D . serum prolactin
- E . short tetracosactide (Synacthen®) test
A 67-year-old woman with type 2 diabetes mellitus presented to the foot clinic with an ulcer at the plantar aspect of her fifth left toe. The ulcer probed to bone but there were no signs of inflammation. There had been a little improvement during 6 weeks of podiatric treatment, but there was some concern about possible osteomyelitis. An X-ray of toe 4 weeks
previously had been normal.
What is the most appropriate next investigation?
- A . CT scan of foot
- B . MR scan of foot
- C . plain X-ray of foot
- D . triple phase isotope bone scan
- E . white cell labelled scan
A 25-year-old woman presented at 28 weeks’ gestation after a screening 75-g oral glucose tolerance test, which had shown a fasting plasma glucose of 5.6 mmol/L (3.0C6.0) and a 2-h plasma glucose of 9.8 mmol/L (<7.8). She had a family history of type 2 diabetes mellitus and a pre-pregnancy body mass index of 36 kg/m2 (18C25). Home blood glucose monitoring had shown persistently raised blood glucose despite dietary modification. She refused insulin because of needle phobia and was concerned about drug exposure to her unborn child.
The use of what hypoglycaemic therapy is acceptable in this situation?
- A . exenatide
- B . glibenclamide
- C . gliclazide
- D . pioglitazone
- E . sitagliptin